

Swallowing Disorders
Normal swallowing is necessary to control one’s secretions as well as to support adequate nutrition.
Normal swallowing is necessary to control one’s secretions as well as to support adequate nutrition.
Voice & Airway Disorders
Using biofeedback, the goal of vocal habilitation is to train each individual to maximize their best vocal quality.
Using biofeedback, the goal of vocal habilitation is to train each individual to maximize their best vocal quality.
Neurogenic Disorders
Neurogenic and motor speech disorders cover a wide variety of disorders that impact one’s speech and language.
Neurogenic and motor speech disorders cover a wide variety of disorders that impact one’s speech and language.
Wellness Your Environment
Group and individual classes offer training to help one become more effective in their individual environments.
Group and individual classes offer training to help one become more effective in their individual environments.
Get Free Initial Consultation
Fees are an estimate only and maybe more depending on your situation.

Rebecca Gould
MS, CCC-SLP, BCS-S
Director/Owner of MedSpeech Inc., Medical Speech-Language Pathologists of the Palm Beaches.

Do you have concerns about your child’s speech and language development?
Early Intervention Leads to Prevention!
It is important to have your child tested and treated as soon as possible if you have concerns or suspect that your child may have any delays or difficulties. A speech-language pathologist (SLP) can help a child with speech and/or language delays. Here at MedSpeech, Inc., we provide a variety of services for the pediatric population including comprehensive diagnostic evaluations and specialized speech and language therapy!
We can provide treatment in a variety of areas including:
- Articulation
- Expressive and Receptive Language
- Social Communication
- Fluency
- Feeding and Swallowing
- Voice
We also provide tutoring services in the areas of reading and literacy. We are currently offering a therapy package: if you purchase 5 therapy sessions for $500 you will receive a complimentary 6th session! Call us today if you have any questions and to schedule your appointment!
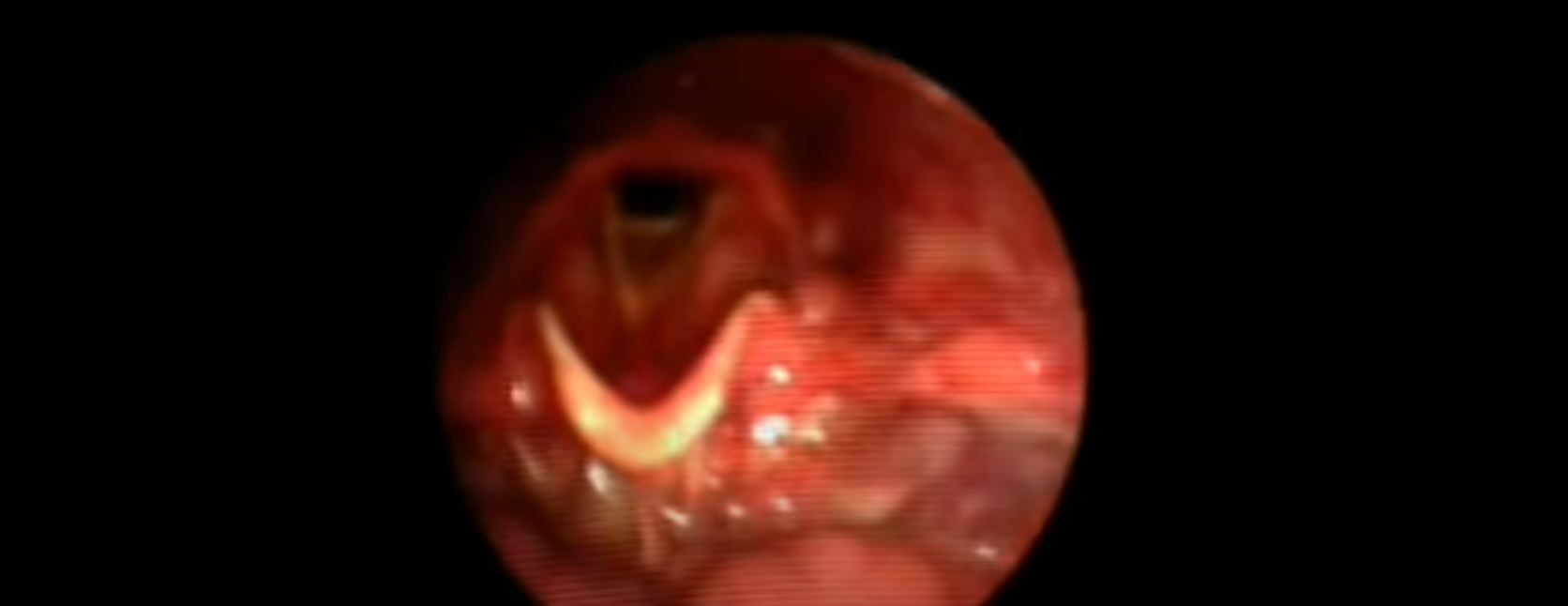
Normal swallow on Fiberoptic Endoscopic Evaluation of Swallowing
Electrical Stimulation & Dysphagia
Neuromuscular electrical stimulation (NMES) is a noninvasive modality that directly stimulates the peripheral nervous system to evoke an action potential via surface electrodes. Physical and occupational therapists have been treating facial paralysis for decades. As early as 1927, physical therapy treatment of Bell’s palsy was advocated using treatment methods that have become “standard” in the decades since…
Testimonials
MedSpeech, Inc., offers a variety of services for all of your speech-language pathology needs. We specialize in:
We also offer fiberoptic endoscopic evaluation of swallowing (FEES) and videostroboscopy. Call us at (561)-833-2090 or click here to fill out our contact form today!